
Slightly more than half of America's senior citizens will need long-term care services either in facilities or within their homes and communities at some point, according to a new national scorecard that questions if most states are up to the job of supporting frail individuals and their families.
By 2026, the oldest baby boomers will begin turning 80, an age when the need for long-term services and support increases. Fifty-two percent of those now turning 65 will eventually require such services or support.
But the ability of states and individuals to meet that need continues to lag behind demographic demand, in spite of some improvements to services and infrastructure, says the report, released Wednesday.
"Where you live matters and it matters because your experience of long-term service and support varies a great deal depending on where you live," said Susan Reinhard, senior vice president of AARP and director of its Public Policy Institute.
Most people cannot afford long-term care services without some government program support. Proposals to cut Medicaid funding are concerning, according to the report's authors, because 60 percent of Medicaid spending goes right now to services for older people with low incomes and those with disabilities.
"Picking Up the Pace of Change: A State Scorecard on Long-Term Services and Supports for Older Adults, People with Physical Disabilities and Family Caregivers" was jointly produced by AARP Foundation, the Commonwealth Fund and the SCAN Foundation.
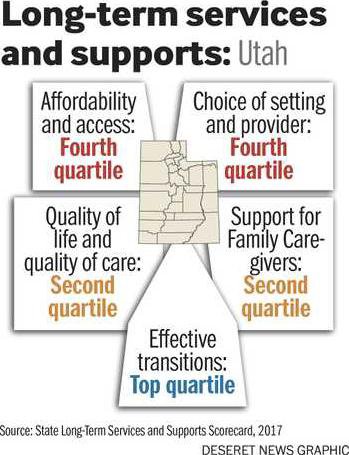
The scorecard ranks states on five categories: whether long-term services and supports are affordable and available; how much choice individuals and families have in who provides care and where; quality of life and care quality; caregiver support; and how patients are transitioned between homes and hospitals and nursing homes. In all, 25 factors were considered within those categories.
Utah ranked No. 24 overall in the report, an improvement from the previous reports. The states' rankings within the categories were divided into fourths, which they refer to as quartiles. Utah fared best in terms of effective transitions, ranking in the top quartile. It hit the second quartile for both support for family caregivers and for quality of life and quality of care. But it was in the bottom quartile in terms of affordability and access and choice of setting and provider.
Long-term services and supports include a broad range of help for those with disabilities, cognitive impairment or health problems. The report includes those who need major care in facilities like nursing homes and those who could remain in their own communities if they had assistance with tasks like getting dressed, bathing, cooking meals, transportation and support for caregiver family members.
Beehive making progress
Utah AARP director Alan Ormsby hailed Utah's ranking as the best state in terms of effective transitions. "That's really positive," he said. "The states does a great job making sure people with low-care needs are not in nursing homes. In Utah, people can successfully transition back into the community."
With passage of the Patient Designated Caregiver Rule, Utah has also "made significant progress in support of family caregivers," he noted. The rule lets someone going into a hospital designate a family caregiver, who is notified when that person is to be discharged or transferred to a different facility. The caregiver can also receive instruction and a demonstration of the care their loved one will need when he returns home.
Caregivers still face major challenges, including that more than 336,000 Utahns provide most of the care unpaid for their aging parents, spouses and others. That unpaid service is worth about $4.2 billion, often provided with little or no outside support.
And Ormsby lamented the improvements still needed in Medicaid home and community-based services. Utah doesn't do as well in making sure older people and those with disabilities can access some needed services outside of facilities, he said.
He believes that Utah's rejection of Medicaid expansion contribute's to the state ranking near the bottom in two areas: Utah ranks 48th in ability to choose where to receive services and from whom. Less than a fourth of funded long-term support and services is targeted to care for people who are older or have disabilities. And the state is No. 46 in the number of home health and personal care aides for every 100 adults who have disabilities.
Besides pushing for Medicaid expansion, Ormbsy said the Utah AARP, which serves more than 221,000 members, hopes to educate the public about who Medicaid serves. "I think there's education that needs to be done to make sure people know who's receiving it and who's at risk if Medicaid is harmed" by proposed national healthcare law changes, he said. "If we expanded Medicaid, there's potential for a number of working poor to improve their situation and find better jobs, too. It's a win-win."
Gaining, losing ground
While the good news is that overall the states have made substantial improvements, compared to previous reports in 2011 and 2014, the gains have been "slow, uneven, incremental change," said Reinhard. "That's not to say it's not important but it's been very slow." She said that fact drove the name of the report, "Picking Up the Pace."
The 2017 report finds huge disparity between the states that are doing the best and those that are the worst. The differences from one place to another are so great, in fact, that Reinhard said it would take 90 years at the current pace for the worst state to do as well as the best state in terms of balancing spending to meet the desire for home and community services compared to nursing home services. It would take 70 years for the worst state to equal the best state in terms of the supply of direct-care workers. Plus, each state had at least one area that needs improvement.
Washington, Minnesota, Vermont, Oregon and Alaska topped the rankings as the best states. The worst are Indiana, Kentucky, Alabama, Mississippi and Tennessee, according to the scorecard. Interestingly, while Tennessee was among the lowest-ranked states, alongside New York it shared a designation as one of the most-improved states.
The greatest improvements made by the states overall since the last report were in reducing the frequency with which those who live in nursing homes are given antipsychotic medications "off label," which means for purposes other than those for which the drug was officially approved and in providing better support for family caregivers, Reinhard said. She noted that 42 states have improved support for caregivers and 48 have reduced off-label use of the drugs.
But more than 20 states also lost ground in terms of the employing people with disabilities, which she called a quality of life and quality of care issue.
Nor did they do well overall in transitioning people who are in nursing homes back into the community when appropriate.
"Twenty-one states have gone backward on that," said Reinhard. "This is a warning sign to me that we are not helping people return to their homes and communities."
And the report said that little or no improvement was made in either the affordability of long-term services and supports or in helping people get them.
It is the first year that housing and transportation have been included in the report. Because some of the factors that make up the report have changed, it's not possible to compare all the rankings from year to year.
States have options
States have "levers" available to make changes, said Gretchen Alkema, vice president of policy and communications for the SCAN Foundation. Among them:
States can update their Medicaid programs to make sure that home- and community-based services are available.
States can "use their licensing and certification authority to marshal a well-trained care delivery workforce" and increase the choices people have in residential settings.
States can emphasize what Alkema calls "age-friendly urban planning" to bolster accessible housing and improve transportation infrastructure.
States also have options to make sure their insurance regulations allow "a range of accessible products."
And they can "repurpose and rethink use of tax dollars and incentives and planning," she said.
One of the biggest challenges, according to Reinhard, is that even individuals, much less states, like to think about long-term care about growing old and the challenges that might come with it which makes it the "step-child" of health and other care systems.
By 2026, the oldest baby boomers will begin turning 80, an age when the need for long-term services and support increases. Fifty-two percent of those now turning 65 will eventually require such services or support.
But the ability of states and individuals to meet that need continues to lag behind demographic demand, in spite of some improvements to services and infrastructure, says the report, released Wednesday.
"Where you live matters and it matters because your experience of long-term service and support varies a great deal depending on where you live," said Susan Reinhard, senior vice president of AARP and director of its Public Policy Institute.
Most people cannot afford long-term care services without some government program support. Proposals to cut Medicaid funding are concerning, according to the report's authors, because 60 percent of Medicaid spending goes right now to services for older people with low incomes and those with disabilities.
"Picking Up the Pace of Change: A State Scorecard on Long-Term Services and Supports for Older Adults, People with Physical Disabilities and Family Caregivers" was jointly produced by AARP Foundation, the Commonwealth Fund and the SCAN Foundation.
The scorecard ranks states on five categories: whether long-term services and supports are affordable and available; how much choice individuals and families have in who provides care and where; quality of life and care quality; caregiver support; and how patients are transitioned between homes and hospitals and nursing homes. In all, 25 factors were considered within those categories.
Utah ranked No. 24 overall in the report, an improvement from the previous reports. The states' rankings within the categories were divided into fourths, which they refer to as quartiles. Utah fared best in terms of effective transitions, ranking in the top quartile. It hit the second quartile for both support for family caregivers and for quality of life and quality of care. But it was in the bottom quartile in terms of affordability and access and choice of setting and provider.
Long-term services and supports include a broad range of help for those with disabilities, cognitive impairment or health problems. The report includes those who need major care in facilities like nursing homes and those who could remain in their own communities if they had assistance with tasks like getting dressed, bathing, cooking meals, transportation and support for caregiver family members.
Beehive making progress
Utah AARP director Alan Ormsby hailed Utah's ranking as the best state in terms of effective transitions. "That's really positive," he said. "The states does a great job making sure people with low-care needs are not in nursing homes. In Utah, people can successfully transition back into the community."
With passage of the Patient Designated Caregiver Rule, Utah has also "made significant progress in support of family caregivers," he noted. The rule lets someone going into a hospital designate a family caregiver, who is notified when that person is to be discharged or transferred to a different facility. The caregiver can also receive instruction and a demonstration of the care their loved one will need when he returns home.
Caregivers still face major challenges, including that more than 336,000 Utahns provide most of the care unpaid for their aging parents, spouses and others. That unpaid service is worth about $4.2 billion, often provided with little or no outside support.
And Ormsby lamented the improvements still needed in Medicaid home and community-based services. Utah doesn't do as well in making sure older people and those with disabilities can access some needed services outside of facilities, he said.
He believes that Utah's rejection of Medicaid expansion contribute's to the state ranking near the bottom in two areas: Utah ranks 48th in ability to choose where to receive services and from whom. Less than a fourth of funded long-term support and services is targeted to care for people who are older or have disabilities. And the state is No. 46 in the number of home health and personal care aides for every 100 adults who have disabilities.
Besides pushing for Medicaid expansion, Ormbsy said the Utah AARP, which serves more than 221,000 members, hopes to educate the public about who Medicaid serves. "I think there's education that needs to be done to make sure people know who's receiving it and who's at risk if Medicaid is harmed" by proposed national healthcare law changes, he said. "If we expanded Medicaid, there's potential for a number of working poor to improve their situation and find better jobs, too. It's a win-win."
Gaining, losing ground
While the good news is that overall the states have made substantial improvements, compared to previous reports in 2011 and 2014, the gains have been "slow, uneven, incremental change," said Reinhard. "That's not to say it's not important but it's been very slow." She said that fact drove the name of the report, "Picking Up the Pace."
The 2017 report finds huge disparity between the states that are doing the best and those that are the worst. The differences from one place to another are so great, in fact, that Reinhard said it would take 90 years at the current pace for the worst state to do as well as the best state in terms of balancing spending to meet the desire for home and community services compared to nursing home services. It would take 70 years for the worst state to equal the best state in terms of the supply of direct-care workers. Plus, each state had at least one area that needs improvement.
Washington, Minnesota, Vermont, Oregon and Alaska topped the rankings as the best states. The worst are Indiana, Kentucky, Alabama, Mississippi and Tennessee, according to the scorecard. Interestingly, while Tennessee was among the lowest-ranked states, alongside New York it shared a designation as one of the most-improved states.
The greatest improvements made by the states overall since the last report were in reducing the frequency with which those who live in nursing homes are given antipsychotic medications "off label," which means for purposes other than those for which the drug was officially approved and in providing better support for family caregivers, Reinhard said. She noted that 42 states have improved support for caregivers and 48 have reduced off-label use of the drugs.
But more than 20 states also lost ground in terms of the employing people with disabilities, which she called a quality of life and quality of care issue.
Nor did they do well overall in transitioning people who are in nursing homes back into the community when appropriate.
"Twenty-one states have gone backward on that," said Reinhard. "This is a warning sign to me that we are not helping people return to their homes and communities."
And the report said that little or no improvement was made in either the affordability of long-term services and supports or in helping people get them.
It is the first year that housing and transportation have been included in the report. Because some of the factors that make up the report have changed, it's not possible to compare all the rankings from year to year.
States have options
States have "levers" available to make changes, said Gretchen Alkema, vice president of policy and communications for the SCAN Foundation. Among them:
States can update their Medicaid programs to make sure that home- and community-based services are available.
States can "use their licensing and certification authority to marshal a well-trained care delivery workforce" and increase the choices people have in residential settings.
States can emphasize what Alkema calls "age-friendly urban planning" to bolster accessible housing and improve transportation infrastructure.
States also have options to make sure their insurance regulations allow "a range of accessible products."
And they can "repurpose and rethink use of tax dollars and incentives and planning," she said.
One of the biggest challenges, according to Reinhard, is that even individuals, much less states, like to think about long-term care about growing old and the challenges that might come with it which makes it the "step-child" of health and other care systems.



